![]()
4 February 2021
How to motivate patients, air-polishing, and online risk assessment – Iain Chapple answers questions on Step 1 of Guideline
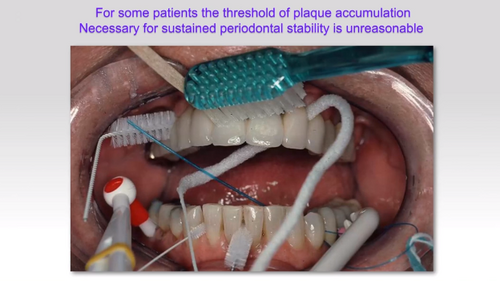
At the end of his EFP Perio Sessions webinar on January 28 addressing Step 1 of the EFP’s S3-level clinical practice guideline for the treatment of stage I-III periodontitis, Iain Chapple addressed a wide range of questions from participants about behavioural change and risk control. Topics covered included patient motivation, air-polishing, flossing, smoking cessation, and the use of online risk-assessment tools.
Q: Are dentists and periodontists really educated to reach our patients correctly? Do we need more lessons, or psychology tricks, to be more predictable in making our patients respect their oral hygiene?
A: A lot depends on experience. If you are a new specialist then clearly you have limited experience, so what can you do to get that patient to engage? I think the key thing is personalising the message. If you show the patient the amount of inflammation on the pocket chart and explain what it means and then show them their radiograph and explain it – give them a journey around their mouth and show them where the bone levels should be and where they are (particularly if the anterior teeth are involved) – that provides them with a powerful visual picture of what is happening in their mouths. That personalisation of the message is really important and using the power of the visual image, the radiograph, to get the message across really helps.
Q: Can you say more about motivational interviewing technique?
A: As periodontal specialists, we are trained in communication or we have a natural ability to communicate. Don’t underestimate our ability to be motivational with our patients. It’s the simple things such as focusing on the things that are working for them and demonstrating to the patient that the bleeding or the pocket depth is reduced in this area and, while it’s not quite where we want it to be, they have made a hell of difference on their own. One of the most powerful messages is, when a patient comes back after Step 2 of treatment and you are doing the review for Step 3 and you can see that there has been a massive improvement, to make sure that the patient understands that they have done that themselves. “You have self-treated” is a line I use all the time. “You are actually eliminating the need for the periodontal specialist by your fantastic home-care regime.” And you need to get them to believe that.
Q: Why is there nothing about air-polishing in the guidelines?
A: When we were planning the workshop [Perio Workshop 2019, which drew up the Guideline], we debated the air-polishing issue because there was some pressure to include it in the systematic reviews. Unfortunately, there was not sufficient evidence for us to be able to do a thorough job of assessing air polishing. The evidence base wasn’t strong enough – there weren’t enough RCTs or systematic reviews to be able to do that – so we made a conscious decision to leave air polishing out of the guidelines. But these guidelines are a live document, and they will need to be updated. I would hope that we would have sufficient evidence from air-polishing studies to be able to address that in the next update to the guideline.
Q: What do you do when treating patient who does not stop smoking? Would you continue with treatment but with fewer treatment aims, or continue with deep scaling until they are motivated to quit smoking?
A: That’s a really good question because it challenges an ethical dilemma. When I was training, we were told not to bother with smokers because they are not going to heal so you are wasting time and you are wasting money. For me, it’s about informed consent. It’s about having the conversation with the smoker whereby they understand that what we do for them physically in terms of our interventions will provide some benefit, but it won’t necessarily result in disease stabilisation and tooth retention unless they stop smoking.
It also depends on your renumeration system. If they are a fee-paying patient it’s their choice, as long as you’ve explained it to them. If you are in the public sector, then can you justify spending public money on someone who is not making an effort to stop smoking? You might have to adopt what I call “palliative periodontal care”, hang on to things for as long as possible without spending too much time with root-surface therapy – and I definitely wouldn’t be doing surgery because they just won’t heal very well and you may make things worse.
Q: Do you believe in developing an online model for self-risk assessment that people can use for seeking treatment and to improve home care?
A: Yes, absolutely. The models are out there. Both the PreViser/DEPPA model and the Lang-Tonetti model have been shown to predict tooth loss. How accurate they are is irrelevant. What is relevant is whether they are effective in the behaviour-change message. If you give a patient a score or show them something visual, does that impact on their belief that they can improve things? If it does then it’s worth using irrespective of its accuracy.
Q: Flossing – should we discard it completely? It is cheaper for patients to buy floss than interdental brushes of different sizes.
A: There has been a tremendous misunderstanding following the primary-prevention workshop [Perio Workshop 2014]. What the systematic reviews showed was that, in a periodontitis patient, dental floss is ineffective because the gaps are too big, and you have to use interdental brushes. What it didn’t do was address the question: if you teach patients to floss, will that prevent the disease from developing? And that’s a really important point. The consensus is that we accept the findings of systematic reviews on a lack of efficacy of flossing, but where the spaces are too tight to use an interdental brush then you should use floss in that situation.
Note: Iain Chapple’s comments have been edited for clarity and concision.
Sign up for our newsletter
The EFP publishes a free monthtly email newsletter with the latest news about the federation's activities, its publications, and its campaigns.
EFP partners
Oral Health Partners:

International & European Association Awards
2021 Winner - European Association of the year